Objectives
Upon completion of this self-study module, the student will be able to:
- Recognize the clinical presentation of croup.
- Describe the approach to the initial management of croup.
- Determine the disposition based on severity of presentation and response to therapy.
Presentation
An 18 month female presents with her mother with complaints of a “barking cough” and “a whistling sound” when she breathes. The patient is audibly stridorous at rest. Vitals: T 38.4 C, HR 140, RR 40, O2saturation 93% on room air.
Introduction
Croup, better known by its formal name of laryngotracheobronchitis, causes subglottic inflammation and edema resulting in laryngeal obstruction and narrowing of the airways. The swelling at the cricoid ring (narrowest part of the pediatric airway) results in symptoms of airflow obstruction (stridor).
Croup is most frequently seen in children age 6 months – 3 years. The most common etiology is parainfluenza although influenza, RSV, or adenovirus can also cause it. The peak incidence of croup is in the fall and winter months.
The clinical features of croup include a 2-3 day history of URI symptoms with progressively worsening cough, especially at night. On day 3 or 4, the classic triad of hoarseness, stridor, and barky cough is heard. The child is usually non-toxic in appearance.
Croup severity can be classified based on the stridor. If there is no stridor, the croup is mild. Croup is considered to be moderate severity if stridor is heard only with exertion or when the child is upset. If there is resting stridor, it is considered severe. Altered mental status or hypoxia in croup indicates impending respiratory failure and is a rare and late finding.
Initial Actions and Primary Survey
As always, start with assessing the ABC’s in a child with difficulty breathing. Assess the airway and the child’s breathing. If there is stridor at rest, the child appears ill, and you think you may need to administer IV steroids or other IV medications, obtain IV access. If stridor is not present at rest and the child is overall well appearing and likely to tolerate oral medications, you may forego the IV initially. Supplemental oxygen is reasonable to start on arrival if respiratory distress is present. Monitoring of pulse oximetry is also useful for repeated assessment in addition to frequent reassessment of clinical status after interventions.
If intubation is needed for severe hypoxia, impending full airway obstruction, or clinically significant altered mental status, you may want to use an endotracheal tube that is one size smaller than usual due to the subglottic narrowing.
Diagnostic Testing
Croup is a clinical diagnosis and an x-ray is not required to make the diagnosis; however, if the diagnosis is not entirely clear or there is suspicion of an alternate cause of the symptoms such as foreign body aspiration, an x-ray of the neck can help differentiate from other causes of upper airway obstruction. The posterior-anterior chest x-ray may show the classic steeple sign in croup, which indicates subglottic narrowing secondary to edema. Overdistention of the hypopharynx with subglottic haziness may be seen on the lateral view. The epiglottis should appear normal and without swelling.
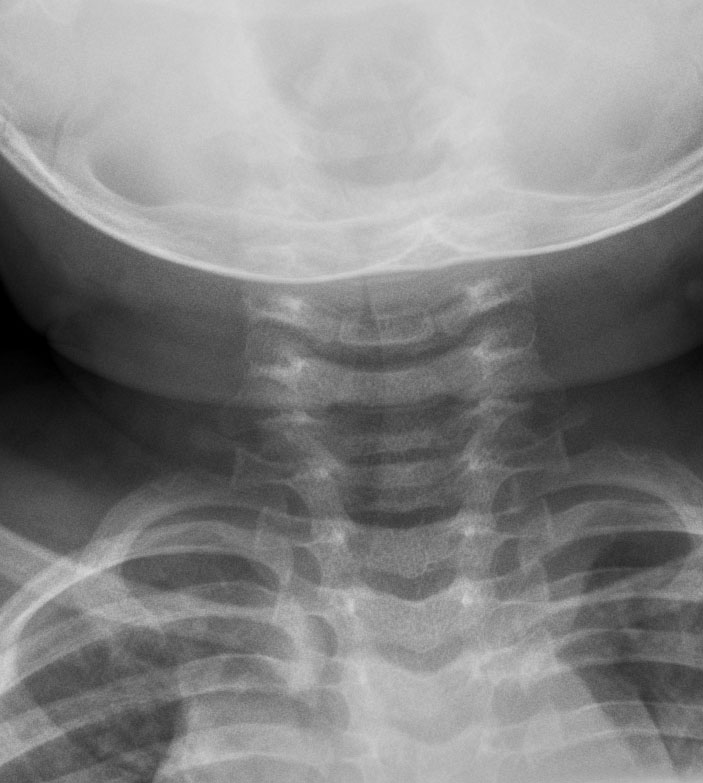
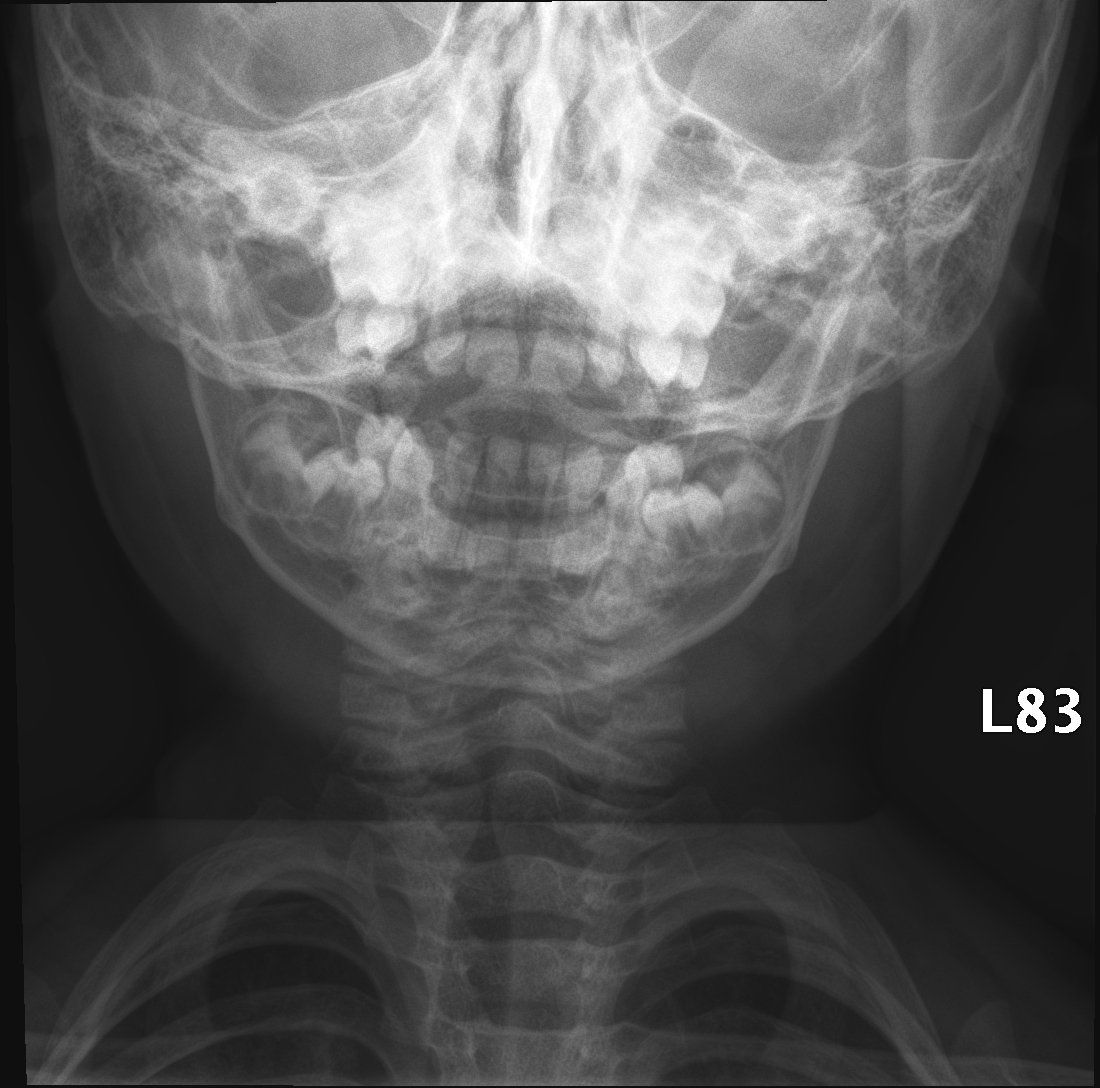
“Steeple Sign”
Pictures courtesy of Dr. Kate Feinstein
Treatment
After airway management and supplemental oxygen, initial treatment includes the following:
Racemic Epinephrine: Any child with severe croup should receive racemic epinephrine. This means anyone with stridor at rest or any patient with croup who appears ill or in distress should be receiving this medication. The dose is 0.5 mL of 2.25% racemic epinephrine in a 2.5 mL normal saline nebulizer. Racemic epinephrine has been shown to reduce length of stay, intubation rates, and ICU admissions. You may repeat dosing every 2-3 hours for a maximum of 3 total consecutive treatments; however, if you are repeating the dose for recurrent stridor after the first dose, admission is likely necessary. You should observe for 3-4 hours after racemic epinephrine administration to assess for return of symptoms and need for admission. If stridor recurs after racemic epinephrine and the child requires another dose, you should admit the child to the hospital.
Dexamethasone: Any child who presents with croup should receive steroids. There is good evidence for decreased admission rates, intubation rates, and ED re-visits if steroids are given. A single dose of dexamethasone is 0.6 mg/kg given as either PO, IV, or IM (effectiveness is the same across preparations). The maximum dose is 10 mg. Repeat doses are not usually recommended.
Alternative therapies: Dexamethsone and nebulized racemic epinephrine are the foundations of therapy. However, some providers treat with prednisolone, prednisone, or inhaled budesonide. Albuterol is not used in the treatment of croup in general.
Disposition
The observation period varies by study and by provider, but it is generally felt that well-appearing croup patients should be observed for a period of time when possible. However, depending on the parents’ comfort level, many children with minimal symptoms who are tolerating PO and have no respiratory distress can be safely discharged home with careful return precautions. In moderate croup, the child should be observed for 2-4 hours after steroids if they remain symptomatic in order to determine disposition – asymptomatic children may be discharged but persistently symptomatic children require admission. If croup is severe and racemic epinephrine is administered, you should observe the child for 3-4 hours for recurrence of resting stridor. If symptoms recur and re-dosing is required, the child should be admitted to the hospital. Other considerations for admission are patients with unreliable parents, children who live far away from the hospital, persistent stridor at rest, previous intubation, other significant comorbid conditions, or significant dehydration.
Criteria for discharge often include:
- No stridor at rest
- Normal pulse oximetry
- Normal color
- Normal level of alertness
- Demonstrated ability to tolerate PO fluids
- Careful return precautions and reliable caregivers
If the child is going home, discuss home management with parents. They may sit by an open window or outside in the cool air to alleviate the symptoms. Humidity such as sitting in the bathroom with the hot shower running may also help. Give careful return instructions and discuss what to expect after discharge. They should follow up with the child’s pediatrician in 24-48 hours.
Differential Diagnosis
- Epiglottitis
- Foreign body aspiration
- Peritonsillar abscess
- Retropharyngeal abscess
- Allergic reaction
- Angioedema
- Bacterial tracheitis
Pearls and Pitfalls
- When in doubt about severity, given racemic epinephrine and observe for 3-4 hours for recurrence of stridor. The biggest pitfall is not observing long enough and discharging the child only to see them back in several hours with recurrent stridor.
- Be sure to discuss what to expect and close follow-up with parents if the child is to be discharged home.
References
- Bjornson CL, Johnson DW. Croup. Lancet 2008; 371:329.
- Cherry JD. Clinical practice. Croup. New England Journal of Medicine 2008; 358:384.
- Fleisher G. Infectious disease emergencies. In: Textbook of Pediatric Emergency Medicine, 5th ed, Fleisher GR, Ludwig S, Henretig FM, Lippincott, Williams & Wilkins, Philadelphia 2006. p.783.
- Kaditis AG, Wald ER. Viral croup: current diagnosis and treatment. Pediatric Infectious Disease Journal1998; 17:827.
- Kairys SW, Olmstead EM, O’Connor GT. Steroid treatment of laryngotracheitis: a meta-analysis of the evidence from randomized trials. Pediatrics 1989; 83:683.
- Ledwith CA, Shea LM, Mauro RD. Safety and efficacy of nebulized racemic epinephrine in conjunction with oral dexamethasone and mist in the outpatient treatment of croup. Annals of Emergency Medicine 1995; 25:331.
- Peltola V, Heikkinen T, Ruuskanen O. Clinical courses of croup caused by influenza and parainfluenza viruses. Pediatric Infectious Disease Journal 2002; 21:76.
- Rizos JD, DiGravio BE, Sehl MJ, Tallon JM. The disposition of children with croup treated with racemic epinephrine and dexamethasone in the emergency department. Journal of Emergency Medicine1998; 16:535.